Getting The Best Shin Splint Treatment in Toronto
We have helped dozens of our practice members recovery from shin splints/medial tibial stress syndrome. We always look to correct the underlying problems that cause any health condition and it is no different for shin splints. To get the best shin splints treatment in Toronto make sure that you seek out a provider that is not just going to Band-Aid the symptoms but fix the underlying cause. Your doctor is going to need to address the tight muscles, irritated nerves, weak glutes and disturbed gait amongst other factors that are often the underlying cause of shin splints.
What Is Medial Tibial Stress Syndrome (MTSS)
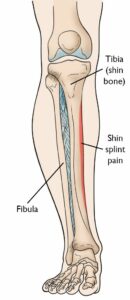
Medial tibial stress syndrome is (one of many) medical terms used for shin splints. MTSS is defined by pain along the posteriomedial (back-inside) border of the tibial that occurs with exercise. It is not pain from an ischaemic (lack of blood flow) origin or signs of stress fracture.
Many of our practice members will say that they have shin splints because of the location of the pain. It is important for your doctor to differentiate between a muscle problem and a bone problem, which we will discuss later. Getting the best shin splint treatment in Toronto will require your doctor to be able to differentiate the underling cause.
How Do I Know If I Have Shin Splints / MTSS?
It is very common amongst runners, military personnel, athletes involved in jumping such as basketball or volleyball players and gymnasts
- One study suggests it occurs 4-6x more common than Achilles tendonitis, iliotibial band friction syndrome, and plantar fascial injuries
- Repetitive running on hard surfaces is common amongst sufferers; increased risk with higher mileage
Symptoms and Signs
- it is a sharp, or profound ache, experienced along the distal half or third of the inside border of the tibia – usually the painful area can be felt right along the bone.
- Pain is felt with activity but generally not with rest
- Initially, pain is not experienced when exercise ceases
- BUT with more chronic cases, symptoms may be felt for a duration of time after you stop the activity that bothers it
- IF you have one or more of the following symptoms, pain, numbness and tingling, cold limb, lack of colour, weakness / paralysis and /or lack of lower limb pulses, then you might have compartment syndrome, which can be a medical emergency
Aetiology: Why Do People Develop MTSS?
It was once thought that traction from the solueos, tibilias posterior and flexor digitorum longus muscles were implicated in causing this injury through their pull on the bony attachment of the tibia
As tension in these aforementioned muscles increases, the tension in the connective tissue fascia around the muscles and the bones increases proportionally. More tension in the muscles causes more tension and repetitive strain on the bone and its connective tissue layer called the periosteum. As many studies have indicated with diagnostic imaging and evaluation, inflammation and pain generation from the periosteum, called periostitis, seems to be implicated.

The symptoms are however, not always felt at the site of origin of these muscles. Often the pain is located lower on the distal 2/3 of the tibial below where these muscles attach.
Research have worked to explain this discrepancy and have also demonstrated that MTSS is not just pain coming from the periosteal fascial bone tissue but also results from bony changes. MTSS is also a bone injury to the outer cortical bone likely resulting from bending of the tibia. Your doctor should know this to provide the best shin splints treatment in Toronto!

Do I Need An X-ray, Ultrasound or MRI?
Imaging studies have shown that there is tibial cortex osteopaenia and, reduced bone mineral density. MRI shows bone marrow oedema (swelling) and periosteal reaction.
When force is put through the tibia at a greater amount or rate than it can adapt to, because of the aforementioned reasons, the bone becomes less dense, more porous and weakens. These bony changes result in pain over time.
MTSS is both a bone and periosteum injury, resulting from a number of causes.
Studies using MRI have shown the MTSS is similar in presentation to a stress fracture but is unlikely to progress to a stress fracture with continued activity. Thus, while MTSS does appear to involve some insult to the bone, I would not recommend complete rest as some would with a fracture. Relative rest from the most insulting activities is likely the best course of action.
My Explanation Of Why We Get MTSS To Patients | Best Shin Splints Treatment in Toronto
Every time that your foot strikes the ground, forces enter into the lower limb and have to be absorbed and dissipated. The harder one strikes the ground (running > walking), the more force that enters and must be accommodated. If the ground reaction force entering the foot, ankle, leg, knee and thigh is not properly absorbed by the muscles, other structures like the ligaments, joints, bones, menisci or tendons will. These structures are less adapt and managing the acute forces that come from exercise, and are likely to sustain a repetitive strain injury if they continue to be exposed to the impact about their tolerance threshold.
When it comes to MTSS there are a number of issues, that are supported in the literature, that I see.
Often there is some sort of combination of the following
- increased ankle mobility / flexibility (why orthotics seem to work) causing the ankle to move with greater pronation or collapse that leaves one prone to this condition
- weakness of the leg muscles (gastroc, soleous, fibularus group, deep calf muscles in some combination)
- weakness of the glutes (gluteus maximus, minimus and medius) causes relative instability of the hip – The hip is not strong enough to control how the thigh, knee and leg move when it hits the ground. Most commonly increased tibial internal rotation or dynamic knee collapse is a consequence of this weakness and likely other muscles attempt to compensate.
- Hyper mobility of the lower limb joints exists, often the superior joint between the tibia and fibula, that further increases the challenge
The result is that the calf muscles, ankle and knee are not properly absorbing the force it accepts when the foot hits the ground. An excessive amount of force is delivered into the deep calf muscles, the tibia and the connective covering of the tibia, which results in a repetitive strain injury.
How We Provide The Best Shin Splints Treatment in Toronto
The key is to ensure the joints, muscles, nerves of the leg are working properly so that the impact forces are accepted by the muscles and not being transmitted to the tibia and its periosteum to perpetuate the injury
How We Achieve This
- Rehab exercise therapy to strength the hip musculature and the muscles of the calf to better stabilize the ankle and knee
- Acupuncture (usually electro-acupunture) to help relieve pain at the site of injury and ensure that the nervous system is working properly to control and power the force dampening muscles
- ART or soft tissue massage to balance the tightness of the lower limb muscle, relieve pain at the site of injury and ensure that when they are asked to, the muscles can slide and contract properly to do their job
- (Kinesio)Taping the lower limb can help up to stabilize the joints of the lower limb and redirect force away from the tibia
- Joint mobilizations and manipulations when needed to ensure better joint movement to correct any joint dysfunctions
- Orthotics when applicable and necessary
The goal is never to just band-aid your pain, but correct the underlying weakness and dysfunctions so that we eliminate the pain and also stop the problem from coming back.
Risk Factors and Causes of MTSS
No single cause has been identified but multiple determinants including, muscle weakness/tightness, hormone imbalance, altered biomechanics and decreased bone density are implicated.
The most common cause of MTSS appears to be abnormal gait (walking) mechanics – most evidence is inferential and lack amazing definitive studies. Disclaimer, there is varying results on the role of many factors (medial arch drop, tibia varum, limb length discrepancy) and MTSS – some of the things may or may not contribute.
- Some evidence that suggests that over-pronation,navicular drop and medial arch-drop (in stance and during running) might be important risk factors inthedevelopmentofMTSS
- arch-drop and pronation are likely to lead to tibial internal rotation during gait; a consequence similar to weak external hip rotators
- Orthotics have been shown to reduce the potential for developing MTSS: confirming that it is related to abnormal gait and foot mechanics
- a study showed that males might be more at risk when they have greater internal and external hip ranges of motion and lower mean catch girth
- lower calf girth and lower muscle volume might result in less strength of the posterior calf muscles to dampen forces being transmitted into the tibia
- calf stretching does not seem to prevent MTSS and ankle dorsiflexion does not seem to be related to its onset
- higher in the female sex
- higher body mass index (BMI) increases the risk
How Do I Know If I Have MTSS For Sure? What Is Needed To Diagnose MTSS?
The diagnosis can be made clinically through a thorough physical examination and history taking. Imagine is not needed to make the diagnosis but may help to rule out other conditions in challenging cases. imaging might demonstrate similar changes in MTSS to stress fracture resulting in false positive diagnoses
- An X-ray is inappropriate in the diagnoses of MTSS unless to rule out a highly suspected stress fracture or other pathologies of concern to your health professional
- A nuclear bone scan maybe useful to confirm a diagnoses BUT are not necessary.
- Often athletes and runners will demonstrate increased bone activity in the legs, detectable on MRI and bone scan that is suggestive of MTSS or a stress fracture, but are completely asymptomatic
- MRI might be useful in determining whether symptoms are due to astressfractureorMTSS.
- However, as with bone scan, MRI shows a high number of false-positive evaluations: In English, many athletes and those susceptible to MTSS, might have MRI signs of MTSS but be completely asymptomatic and not develop MTSS
References
Moen, Maarten H., et al. “Medial tibial stress syndrome.” Sports medicine 39.7 (2009): 523-546.
Michaud, Thomas C. Human locomotion: the conservative management of gait-related disorders. Newton Biomechanics, 2011.