Your Knee Pain Is Not A Knee Problem

If you are active and have never had a knee injury, you are in the minority. Be thankful. If you are like me and the rest of us, you have had a knee problem at some point in your life!
I can fully attest to this! During my athletic career, my knees have stopped me from training for a half / full marathon, cut short a bike ride and made a few too many hockey games less enjoyable… and it sucks!
Hopefully, like me, you have been lucky enough to avoid a serious knee injury that has resulted in any permanent damage to the knee. Rupturing the ACL, tearing of a meniscus or sprain of one of the other major ligaments are serious injuries but are thankfully rare.
Like most people that have recurrent knee pain, my issue, and the issue of so many runners, cyclists, football, basketball and soccer players, is a repetitive strain injury.
Repetitive strain injuries (RSI) of the knee are so common that they affect about 25% of runners every year! There are many diagnoses that you have likely been labelled with or have heard: iliotibial band syndrome (ITB syndrome), patellofemoral pain syndrome (PFPS), bursitis of many kinds, medial-joint line irritation, osteoarthritis, meniscal strain, and fat-pad syndrome to name a few.
All of these conditions and more receive their very own section in the textbook with a special diagnosis and orthopaedic tests. They are treated as exclusive and separate entities by practitioners and researchers alike.
But what not a lot of people are talking about, and what you have likely never been told, is that the SOURCE OF THE PAIN and the ACTUAL PROBLEM causing that pain is the same for all of these conditions.
Before we launch straight into it, let us take a step back to first principles and just address what happens when we walk, run or sprint.
When we strike the ground with the foot and ground reaction forces travel up through the lower limb, these forces have to be dissipated and absorbed. Under optimal circumstances, the bones, ligaments, and most importantly the muscles, act to absorb the force of the ground to evenly distribute them.
If a particular tissue is exposed to a higher amount of ground reaction force than it is adapted to handle, it can cause a microscopic injury to that tissue.
Now let’s say that you go for a run or a bike ride for a higher intensity or a longer duration than you normally would. The cells and tissues that make up the bones, ligaments, muscles, and joints are forced absorb more force than they are used to and with each repetitive motion, more and more damage is done to the most overstressed tissue.
If there is an uneven and greater than normal force being absorbed by the ligaments on the inside of the knee, this will likely result in a microscopic tearing, pain, and sidelined athlete.
This tissue overload can be the result of too much training, too quickly; training for a marathon in a month when you have not run before.
They are more commonly the result of relative muscle weakness or a faulty movement pattern that overloads a particular bone, muscle or ligament; too much force being absorbed by too weak a tissue.
For military recruits, one of the most common RSI is a stress fracture of a toe. Too much force, repeatedly loaded onto an unadapted foot, in a bad shoe, too quickly.
SO BACK TO THE KNEE
Despite being a relatively simple hinge joint for all intents and purposes, the knee is so commonly injured with activity!

The knee is well adapted to flex and extend like a door hinge moving around an axis of rotation – back and forth – back and forth. When it is forced to accept a lot of rotation or side-to-side (lateral) bending forces that shear or twist its hinge pattern, it is more likely to be injured.
Unfortunately, almost every single sport and activity requires some lateral movement of the body and the knee. Thus, we are required to minimize the amount of lateral force entering into the knee and absorb it or be constantly injured and sidelined.
We reduce the amount of force entering the body by simply wearing shoes. The only way to change how we absorb that force that enters through the shoes is to change how our muscles fire and our joints move.
But if the knee is not meant to absorb a lot of side-to-side movement because of its hinged design, what is the body to do?
Thankfully that is what the ankle and the hip are designed for.
An assortment of studies on RSIs of the knee, and even those on hip injuries like arthritis, hip bursitis, and sacroiliac joint pain, all point back to hip weakness as the underlying cause. And by hip, these studies mean your glutes! Weakness in the glutes is the ACTUAL PROBLEM.
This is especially true of PFPS/Runners Knee where the foremost research has demonstrated that weakness or movement dysfunctions at the hip and ankle are often more related to this condition than what is happening at the knee.
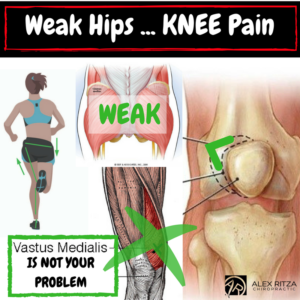
The hip musculature (glutes, TFL, obliques, etc) is larger and more powerful than that of the knee and is better able to accept ground reaction forces. Furthermore, the activity of these muscles at the hip, dictate where and how the knee moves. Like the ball and socket joint of the shoulder controlling where the elbow goes, the hip muscles point the knee in the right direction and keep it there.
When we run, the hip muscles should point the knee straight forward and keep the body aligned overtop of it; not collapsing inward because of hip muscle weakness.
MRI findings have demonstrated that symptoms related to knee pain result from increased side-to-side shear forces at the knee as a result of hip muscle weakness; in English, this means the knee is translating and rotating too much left-and-right, rather than just forward and back. This leads to RSI and knee pain.
Rather than using the powerful muscles of the hip to control the knee, absorb lower limb ground reaction forces and maintain balance, injury prone athletes tend to use the muscles of the knee and leg. Using the muscles around the knee to absorb force is called a knee-strategy.
We mistakenly use a knee-strategy rather than a hip-strategy. As told by Dr. Chris Powers at a recent conference, a leading researcher on knee and lower extremity injuries, we are more adverse to injury when we adopt a hip strategy. Activating and using the gluteal muscles of the hip will help to rehabilitate an injured knee and reduce the incidence of future injury.
So what is the SOURCE OF THE PAIN?
In every case, there is a slight variation in what part of the knee joint is irritated. Whether it is the meniscus, ligament, cartilage, bursa or joint-capsule is relatively unimportant as long as there is no major tearing involved.
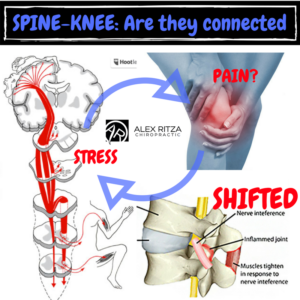
It is unimportant because the source of the pain is always your nervous system and that is what has to be corrected and managed. The nervous system is what sends the signal to your brain that there is a painful problem. Chronic changes in the nervous system are what leads to chronic pain in the long term after the tissues have healed.
The body is exceptional at healing itself and will heal whatever knee joint tissues are affected with enough rest. The major concern following a repetitive strain injury of the knee is the compensatory changes that happen in the nervous system as a result.
Following a knee injury, the nervous system goes into “crises lockdown mode” whereby it reduces the strength of the signal it sends to the muscles of the lower limb, making them weaker, and changes the strategy it uses to stabilize the knee. It will naturally and unconsciously adopt a knee-strategy instead of a hip-strategy to compensate for the injury. We know that this is counterproductive in the long term.
The situation is further worsened by the fact that the changes do not often completely reverse themselves after the pain has resolved. The nervous system gets stuck in this “crises lockdown mode” until it is specifically addressed.
Most knee injuries become chronic and repetitive not because of the initial injury to the tissue that has since healed, but because the nervous system itself never healed. The power supply to the knee was never turned back on and there will be ongoing weakness and an altered strategy to stabilize the knee until this change is reversed.
Strengthening the hips and using a hip-strategy to stabilize the knee is paramount! But if the power supply to the hip and knee is not restored, it is going to be very challenging to function even close to optimally.
We highly encourage you to download and enjoy our FREE – HIP STRATEGY PROTOCOL LEVEL 1 GUIDE to start to build your hip strategy and strengthen the muscles of the hip and core.
If you have chronic knee problems they could be the result of a CORE PROBLEM with your spine and nervous system. Core problems in the spine and nervous system can lead to some obvious health changes you are aware of, and some you have no idea about…. including your knees.
If the hip strategy is not enough for you, schedule a Complimentary Case Review with us to begin to investigate if there is more going on than just your sore knee.
Dr. Alex